About
The Michigan Barrett's Esophagus pREdiction Tool (M-BERET)
The M-BERET estimates the probability that an individual aged 40-79 years old has Barrett's esophagus. Barrett's esophagus is a change in the lining of the esophagus (swallowing tube) that is associated with an increased risk of developing cancer of the esophagus (esophageal adenocarcinoma). However, the vast majority of people with Barrett's esophagus never develop cancer of the esophagus.
The M-BERET was developed from the Newly Diagnosed Barrett's Esophagus Study conducted at the University of Michigan and the Ann Arbor Veterans Affairs Medical Center1 and has subsequently been validated.2,3,4 This tool is intended to be used by health professionals. If you are not a health professional, please discuss your risk with your doctor.
The M-BERET is not intended for use in individuals who have previously undergone upper endoscopy. It is also not intended for use in individuals with difficulty swallowing (food getting stuck), unintentional weight loss, or bleeding. Such symptoms may warrant endoscopy regardless of the predicted probability of Barrett's esophagus.
Questions
What is the patient's sex?
What is the patient's age?
Heartburn is "
a burning sensation in the chest, behind the breastbone, that rises up toward the neck or mouth."
Regurgitation is "
the effortless movement of stomach contents up into the chest, throat, or mouth."
Have you smoked at least 100 cigarettes in your life?
What was the most you have smoked per day?
OR
waist circumference
While wearing only underwear or a hospital gown, and standing erect, palpate the hip area to locate the bony right ilium (Figure). Repeat on the left side. Place a soft measuring tape around the trunk in a horizontal plane at the levels of the iliums on both sides of the trunk. This is typically near the level of the umbilicus. Hold the zero-end below the measurement value. Check for horizontal alignment of the measuring tape in front and back. Make sure that the tape is snug, but does not compress the skin. Measure to the nearest 0.1 cm. Repeat the measurement to make sure it is correct.
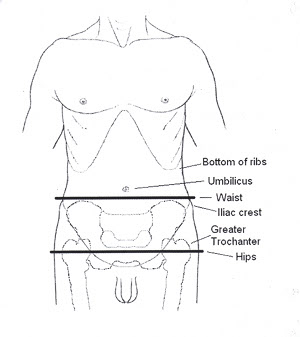
hip circumference
Measure while standing erect, with feet together, and weight evenly distributed on each foot.
Feel the greater trochanters of the hips (Figure). While making sure the tape remains horizontal, find the maximum circumference, including the buttocks and greater trochanters. Keep the tape snug, without compressing the skin. Make the measurement to the nearest 0.1 cm. Repeat the measurement to make sure it is correct.
References
References
1. Rubenstein JH, Morgenstern H, Appelman H, Scheiman J, Schoenfeld P, McMahon L, Metko V, Near E, Kellenberg J, Kalish T, Inadomi JM. Prediction of Barrett's Esophagus among Men with and without GERD Symptoms. American Journal of Gastroenterology 2013;108:353-62.
2. Thrift AP, Vaughan TL, Anderson LA, et al. External Validation of the Michigan Barrett's Esophagus Prediction Tool. Clin Gastroenterol Hepatol 2017;15:1124-1126.
3. Rubenstein JH, McConnell D, Waljee AK, Metko V, Nofz K, Khodadost M, Jiang L, Raghunathan T. Validation and Comparison of Tools for Selecting Individuals to Screen for Barrett's Esophagus and Early Neoplasia. Gastroenterology. 2020;158:2082-2092
4. Rubenstein JH, Raghunathan T, Doan C, Schneider J, Zhao W, Metko V, Nofz K, Khodadost M, Corley D. Validation of Tools for Predicting Incident Adenocarcinoma of the Esophagus or Esophagogastric Junction. American Journal of Gastroenterology. 2021;116(5):949-957.
5. Desai TK, Krishnan K, Samala N, Singh J, Cluley J, Perla S, Howden CW. The incidence of oesophageal adenocarcinoma in non-dysplastic Barrett's oesophagus: a meta-analysis. Gut 2011:published on October 13, 2011 as 10.1136/gutjnl-2011-300730.
6. Muthusamy VR, Wani S, Gyawali CP, Komanduri S, Bergman J, Canto MI, Chak A, Corley D, Falk GW, Fitzgerald R, Haidry R, Inadomi JM, Iyer PG, Konda V, Montgomery E, Ragunath K, Rubenstein JH, Samarasena JB, Schnoll-Sussman F, Shaheen NJ, Smith M, Souza RF, Spechler SJ, Trindade A, Yapp RG. AGA Clinical Practice Update on New Technology and Innovation for Surveillance and Screening in Barrett's Esophagus: Expert Review. Clinical Gastroenterology and Hepatology. 2022;20(12):2696-2706.